
Obstetrics and Childbirth
Pre-Eclampsia & Eclampsia
Vaginal Bleeding
Obstetrical Transportation Destination
Newborn Resuscitation
Apgar Score
Abandoned Newborn
General Considerations for Pregnant Patients
- Determine the date of the last menstrual period (LMP) and approximate weeks gestation
- Patients in the late 2nd or 3rd trimester (>28 weeks) should be transported in a left lateral recumbent position (including those immobilized on a back board) to avoid compression of the inferior vena cava by the gravid uterus
Childbirth
Basic Life Support
- Supplemental oxygen
- Including ETCO2 level (35-45 normal)
- Do not place fingers or hand inside birth canal for assessment
- If presenting part is not the head (i.e. foot, arm, or buttock first) immediately begin transport to the nearest OB facility; continue supportive care en route
- Delivery:
- Slow, controlled delivery of head; apply gentle perineal pressure
- If the umbilical cord is wrapped around the child’s neck, gently unwrap prior to completion of delivery
- Observe for and document meconium staining
- Following delivery, follow newborn resuscitation protocol
- Double clamp cord 10-12 inches from abdomen
- Cut cord between clamps
- Maintain body temperature
- Allow spontaneous delivery of placenta; do not apply traction to umbilical cord for placental delivery
- If placental delivery occurs, package in biohazardous waste bag and hand over to hospital staff upon arrival
- Slow, controlled delivery of head; apply gentle perineal pressure
- Postpartum:
- For newborn, see newborn resuscitation protocol
- Assess for postpartum hemorrhage
- Gently massage abdominal wall overlying the uterine fundus until firm
- Transport to nearest OB receiving facility
Advanced Life Support
- For mom if condition warrants
- Full ALS Assessment and Treatment
- See newborn resuscitation protocol
Pre-eclampsia & Eclampsia
Pregnancy induced hypertension, pre-eclampsia and eclampsia are conditions typically encountered in late 2nd or 3rd trimester pregnancy, and( less commonly) in the postpartum periods (up to 2 months). Clinical manifestations may include elevated blood pressure (SBP > 160mmHg or DBP > 120 mmHg), headache, peripheral edema, confusion, agitation or seizures.
Advanced Life Support
- Full ALS Assessment and Treatment
- If the patient is ≥ 20 weeks pregnant (third trimester), administer Magnesium Sulfate 4 grams IV over 10 minutes for either of the following:
- Systolic BP > 160 mmHg or Diastolic BP > 120 mmHg on two readings
- Active seizures
- If the patient is < 20 weeks pregnant or post-partum, and Magnesium is being considered, contact Medical Control for orders
- FOR ACTIVE SEIZURES, REGARDLESS OF NUMBER OF WEEKS PREGNANCY:
- Midazolam (Versed) 5 mg IM or intranasal via MAD OR 2.5mg IV
- If seizures continue or re-occur repeat Midazolam (Versed) 5 mg IM or intranasal via MAD OR 2.5 mg IV; wait at least 5 minutes from initial dose
- Do NOT delay treatment to obtain intravenous access, begin with IM dose unless IV is already established.
- Blood glucose measurement
- If < 70 mg/dL administer
- Dextrose 10% 100ml IV/IO, (repeat in 10 minutes if BGL remains < 60 mg/dl) max of 250ml
- See General Illness protocol for additional detail
- If < 70 mg/dL administer
Vaginal Bleeding
- A visual inspection of the vaginal area to look for crowning or presenting parts is appropriate, but do not place fingers or hand inside birth canal during assessment
- 1st or 2nd Trimester or unknown pregnancy status
- Position of comfort
- 3rd Trimester Bleeding (≥ 26 weeks)
- Left Lateral recumbent position
Advanced Life Support
- If bleeding moderate or heavy perform Full ALS Assessment and Treatment
- If gestational age known to be < 20 weeks transport to closest hospital
- If gestational age known or possibly > 20 weeks transport to closest OB receiving facility
- Transport any products of conception or fetal material present at the scene to the receiving facility
Contact Medical Control for Additional Orders if Needed
Obstetrical Transport Destination
If delivery is not imminent and patient is stable, transport to patients requested obstetric (OB) receiving facility.
Patient known to be < 20 weeks gestation:
- 1st day of last menstrual period < 20 weeks ago
- Available information verifying gestational age < 20 weeks (e.g. known due date)
- Transport to closest emergency department (not closest obstetric facility)
Patient known to be >= 20 weeks gestation:
- abnormal delivery presentation transport to the nearest OB receiving facility
- Imminent delivery or medically unstable mother
- Transport to nearest ED
- Non-traumatic abdominal, pelvic or back complaints, vaginal bleeding/spotting or any vaginal fluid leak or discharge
- Transport to closest OB receiving facility
- Patient's preference should be considered if condition allows
- Includes minor trauma patients
- Transport to closest OB receiving facility
Pregnancy & Trauma
- Transport all pregnant patients meeting Trauma Alert criteria to a State Approved Trauma Center
- Trauma Yellow can be transported to State Approved Trauma Center per Paramedic judgment
- Trauma Green can be transported to ED of closest OB receiving facility
- If < 20 weeks gestational age, minor trauma patients can be transported to nearest ED
- If abdominal pain or vaginal bleeding with significant mechanism (ex. MVC > 35 mp, steering wheel deformity, fall onto abdomen) and pregnancy > 20 weeks, trauma alert and transport to a State Approved Trauma Center
OB Receiving Facilities
Advent Health Celebration
Advent Health Orlando
Osceola Regional Medical Center
Winnie Palmer Hospital
Holmes Regional Medical Center (Melbourne)
Heart of Florida Regional Medical Center (Haines City)
Lawnwood Regional Medical Center
Indian River Medical Center
Contact Medical Control for Additional Orders if Needed
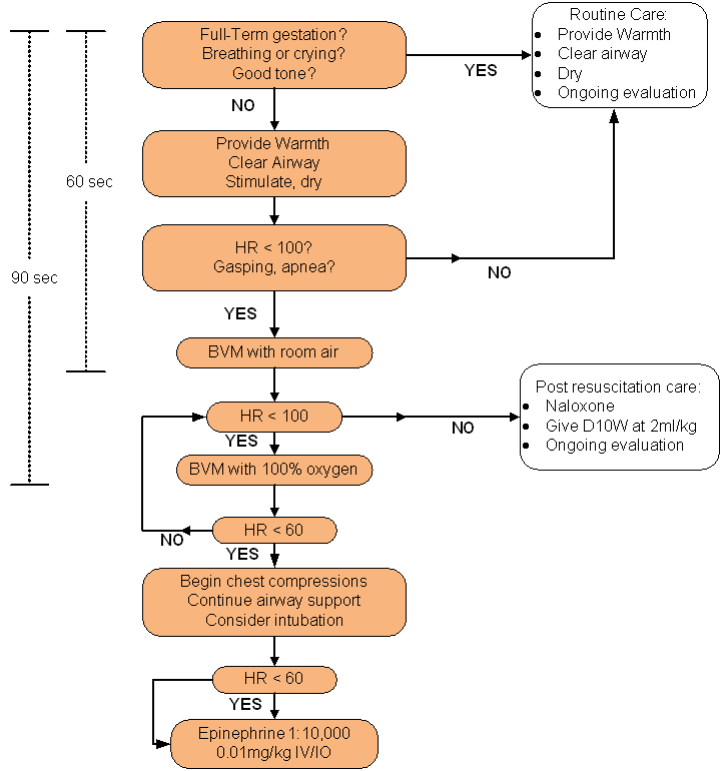
Newborn Resuscitation
Basic Life Support
- Note gestational age, and if twin gestation is known
- Assess for presence of meconium
- Assess breathing or presence of crying
- Assess muscle tone
- Assess color
- Provide warmth
- Spontaneously breathing, well-appearing infants do not require suctioning
- For infants who have obvious obstruction to spontaneous breathing or who require positive-pressure ventilation, open airway and suction with bulb syringe
- Suction mouth first, then nasopharynx
- Dry, stimulate and reposition
- Administer supplemental blow-by oxygen
- Evaluate respirations, heart rate, and color
- If apnea, or HR < 100, provide ventilations using BVM and room air initially
- If HR remains < 60, begin chest compressions
- Note APGAR scores at 1 and 5 minutes after birth and then sequentially every 5 minutes until VS have stabilized
Advanced Life Support
- If the fluid contains meconium and the newborn has absent or depressed respirations, decreased muscle tone, or heart rate < 100 bpm:
- Suction any visible meconium from the hypopharynx and airway
- After suctioning, provide ventilations using BVM and 100% Oxygen
- If apnea, or HR < 100, provide ventilations with 100% Oxygen
- Target oxygen saturation after birth:
- 1 min – 60-65%
- 2 min – 65-70%
- 3 min – 70-75%
- 4 min – 75-80%
- 5 min – 80-85%
- 10 min – 85-95%
- If HR remains < 60, administer chest compressions
- Administer boluses of 0.9% NaCl at 20ml/kg
- If no IV access obtained after 3 attempts, or within 90 sec., obtain IO access
- Epinephrine 0.01 mg/kg IV of a 1:10,000 solution if no improvement
- Repeat Epinephrine (same dose) every 3 to 5 minutes if no response
- Naloxone (Narcan) 0.1 mg/kg, IV or IO if respiratory depression in a newborn of a mother who received narcotics within 4 hours of delivery
- Repeat Naloxone (Narcan) dose as needed
- Administer D10W at 2ml/kg; no need to check blood glucose prior to administration
- Administer boluses of 0.9% NaCl at 20ml/kg
Note: The tracheal suctioning procedure is not intended for the vigorous newborn with meconium stained fluid that does not develop apnea or respiratory distress.
APGAR Score
APGAR is a quick test performed at 1 and 5 minutes after birth. The 1-minute score determines how well the baby tolerated the birthing process. The 5-minute score assesses how well the newborn is adapting to the new environment. The rating is based on a total score of 1 to 10, with 10 suggesting the healthiest infant. This test is a screening tool to help determine whether a newborn needs resuscitative efforts.
|
0 (Points) |
1 |
2 |
|
|
Appearance |
Blue or pale all over |
Blue extremities, but torso pink |
Pink all over |
|
Pulse |
None |
< 100 |
≥ 100 |
|
Grimace |
No Response |
Weak grimace when stimulated |
Cries or pulls away when stimulated |
|
Activity |
None |
Some flexion of arms |
Arms flexed, legs resist extension |
|
Respirations |
None |
Weak, irregular or gasping |
Strong Cry |
| 0-3 Critically Low, 4-6 Fairly Low, 7-10 Generally Normal | |||
Abandoned Newborn
Florida Statute 383.50 allows for new parents to anonymously leave a newborn at a fire station or a hospital. If this scenario is encountered, adhere to the following:
- Assess and treat the newborn as per newborn/pediatric resuscitation protocols
- Transport newborn to nearest emergency department
- If possible record physical description of parent
- Attempt to obtain information regarding prenatal care and pertinent family history
- If any written information available, turn it over to the Emergency Department
Contact Medical Control for Additional Orders if Needed