Adult Cardiac
Cardiac Arrest General Approach
Asystole
Pulseless Electrical Activity
Ventribular Fibrillation/Pulseless V-Tach
Cardiac Arrest - Post Resuscitation Care
Cardiac Arrest - Termination of Resuscitation (Medical)
Cardiac Arrest - No Resuscitation Attempt
Atrial Fibrillation or Flutter
Bradycardia
Supraventribular Tachycardia
Wide Complex Tachycardia
Polymorphous VT (Torsades)
Chest Pain - Suspected Cardiac Ischemia
Ventricular Assist Device (VADs)
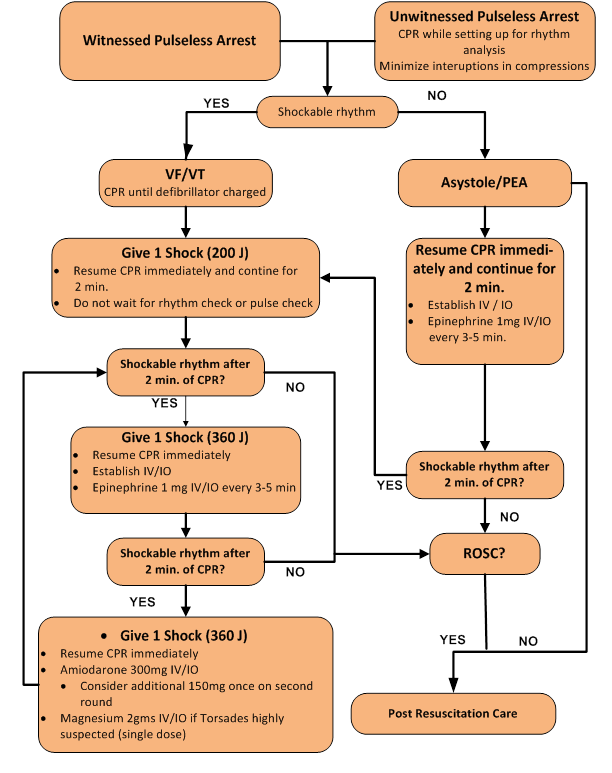
Cardiac Arrest General Approach
In the event a patient suffers cardiac arrest in the presence of EMS, the absolute highest priority is to apply the AED/Defibrillator and deliver a shock immediately if indicated. In the setting of cardiac arrest not witnessed by EMS, perform CPR immediately and continuously while setting up for rhythm analysis and delivery of shocks. If shockable rhythm present, deliver shock without delay.
The first 5 minutes of CPR shall be done manually (this does not include on scene bystander CPR). Mechanical CPR devices can be used only if there is no delay in applying the device. If a delay in applying the device occurs, continue manual compressions immediately.
Adult medical cardiac arrest patients should be resuscitated on scene for at least 20 minutes, unless the patient is in refractory ventricular fibrillation/ventricular tachycardia (4th shock delivered and remains in V-fib/V-tach, initiate transport).
Basic Life Support
- Check responsiveness
- Call “Patient Contact/Working code” time to dispatch
- Utilize pit crew approach (see procedure pg. ___)
- Open airway, check breathing, and feel for carotid pulse
- If a pulse is not definitely felt within 10 seconds immediately begin chest compressions while preparing to apply AED or Monitor/Defibrillator
- Assist ventilation with minimal interruptions in chest compressions
- 30:2 compression to ventilation ratio for BLS
- Apply AED and follow directions
- If shockable rhythm identified by AED:
- Administer shock and call “first shock” time to dispatch
- Resume CPR immediately after shock is delivered for 2 minutes
- Do not wait for pulse or rhythm check
- Re-analyze rhythm using AED and follow directions
- Continue assisted ventilation without chest compressions if pulse present
Advanced Life Support
- Advanced airway/ventilatory management
- Ventilation rate of 8-10 per minute (avoid hyperventilation)
- If unwitnessed arrest, immediately begin CPR and continue until ready for rhythm analysis
- Follow algorithm for specific rhythm
- Attempt peripheral IV, if unobtainable proceed to adult intraosseous access
- All medications listed for IV use can be given IO
- When available, give 1 amp (25 g) of D50 for hypoglycemia in cardiac arrest
Important Principles for Cardiac Arrest Management
- Minimize interruptions in chest compressions
- Compressions should begin immediately upon identifying pulselessness
- Compressions should be continuous (no pause for ventilations, airway management)
- Minimize interruption time in compressions
- Have 2nd provider ready to initiate compressions side by side
- Deliver shocks in VF/VT and whenever possible, continue CPR while defibrillator is charging
- Avoid hyperventilation (use rate of 8-10 breaths/minute)
- Capnography is required on every patient with an ETT or SGA in place
- Allows rapid assessment of ROSC (marked by a sudden increase in ETCO2 value, typically an increase of 10 mmHg)
- Consider the H's and T's that may have caused the arrest
- Management of medical cardiac arrest patients should be performed on scene for 20 minutes prior to transport, barring any safety issues. Time zero begins with initiation of resuscitation by engine or rescue
|
H’s |
T’s |
|
Hypoxia |
Toxins |
|
Hypovolemia |
Tamponade (Cardiac) |
|
Hydrogen Ion (Acidosis-prolonged down time does not apply here) |
Tension pneumothorax |
|
Hyperkalemia |
Thrombosis, pulmonary |
|
Hypothermia |
Thrombosis, coronary |
Contact Medical Control for Additional Orders if Needed
Cardiac Arrest - Asystole
When asystole is seen on the cardiac monitor confirmation of the rhythm shall include a printed rhythm strip, as well as interpretation of the rhythm in more than one lead. Low amplitude V-Fib or PEA may be difficult to distinguish from asystole when using only the cardiac monitor display for interpretation.
Advanced Life Support
- Follow Cardiac Arrest-General Approach protocol
- Consider and treat possible causes (see H’s and T’s)
|
Potential Cause of Asystole |
Treatment |
|
Hypovolemia (most common cause) |
|
|
Hypoxia |
|
|
Hydrogen ion, acidosis (prolonged down time does not apply here) |
|
|
Hyperkalemia (end stage renal disease/dialysis) |
|
|
Hypothermia |
|
|
Toxins (drug overdose) |
|
|
Tamponade, cardiac |
|
|
Tension pneumothorax (all blunt trauma in cardiac arrest) |
|
|
Thrombosis, coronary |
|
|
Thrombosis, pulmonary |
|
- Epinephrine 1:10,000 1 mg IV/IO every 3-5 min during arrest
- Drug overdoses (see specific drug OD/toxicology section)
- Calcium Chloride 1 gram IV/IO for calcium channel blocker OD
- Avoid if patient on Digoxin / Lanoxin
- Calcium Chloride 1 gram IV/IO for calcium channel blocker OD
- Sodium Bicarbonate 1 mEq/kg IV/IO for Tricyclic antidepressant OD (max 50 mEq)
- Naloxone (Narcan) 2 mg IV/IO for possible narcotic OD; may also be given IM or via Mucosal Atomizer Device (MAD)
- If no response to resuscitative efforts in 20 minutes (at least 2 rounds of drugs) consider discontinuation of efforts (see “Termination of Resuscitation” protocol)
Contact Medical Control for Additional Orders if Needed
Cardiac Arrest - Pulseless Electrical Activity
Advanced Life Support
- Follow Cardiac Arrest-General Approach protocol
- Consider and treat possible causes:
|
Potential Cause of PEA |
Treatment |
|
Hypovolemia (most common cause) |
|
|
Hypoxia |
|
|
Hydrogen ion, acidosis (prolonged downtime does not apply here) |
|
|
Hyperkalemia (end stage renal disease, dialysis) |
|
|
Hypothermia |
|
|
Toxins (drug overdose) |
|
|
Tamponade, cardiac |
|
|
Tension pneumothorax (all blunt trauma cardiac arrest) |
|
|
Thrombosis, coronary |
|
|
Thrombosis, pulmonary |
|
- Epinephrine 1:10,000 1 mg IV/IO every 3-5 min during arrest
- Drug overdoses (see specific drug OD/toxicology section)
- Calcium Chloride 1 gram IV/IO for calcium channel blocker OD
- Avoid if patient on Digoxin / Lanoxin
- Calcium Chloride 1 gram IV/IO for calcium channel blocker OD
- Sodium Bicarbonate 1 mEq/kg IV/IO for Tricyclic antidepressant OD (max 50 mEq)
- Naloxone (Narcan) 2 mg IV/IO for possible narcotic OD; may also be given IM or via Mucosal Atomizer Device (MAD)
- Repeat every 3-5 minutes (Maximum 8 mg)
Contact Medical Control for Additional Orders if Needed
Cardiac Arrest - Ventricular Fibrillation/Pulseless V-Tach
Advanced Life Support
- Follow Cardiac Arrest-General Approach protocol
- Defibrillate for persistent VF/VT:
- 200 J for initial biphasic shock, 360 J for subsequent shocks
- Continue CPR immediately after shock (do not stop to check pulse or rhythm)
- Call first defibrillation time to dispatch (if not done above)
- Analyze rhythm after 2 minutes of good CPR; If VF/VT persists:
- Defibrillate at 360 J
- Continue CPR immediately after shock (do not stop to check pulse or rhythm)
- Epinephrine 1:10,000 1 mg IV/IO every 3-5 min during arrest
- Analyze rhythm after 2 minutes of good CPR; If VF/VT Persists:
- Defibrillate at 360 J
- Continue CPR immediately after shock (do not stop to check pulse or rhythm)
- Amiodarone 300 mg IV/IO bolus
- For persistent VF/VT give Amiodarone 150 mg IV/IO bolus on second round
- Or consider Lidocaine
- Lidocaine IV/IO initial dose: 1–1.5 mg/kg
- If persistent VF/VT then Lidocaine IV/IO repeat dose: 0.5–0.75 mg/kg every 5 to 10-minutes with maximum cumulative dose of 3 mg/kg
- Follow with continuous infusion of 1 to 4 mg/minute after return of perfusion
- Lidocaine IV/IO initial dose: 1–1.5 mg/kg
- Continue cycle of CPR & Drug ----> Rhythm Check ----> CPR ----> Shock ----> CPR and Drug ----> Rhythm Check ----> CPR ----> Shock as needed
- Additional interventions to consider in special circumstances:
- Magnesium Sulfate 2 g IV/IO push over 1-2 minutes only if suspected Polymorphous VT (torsades de pointes) or hypomagnesemic state (chronic alcohol, diuretic use)
- Sodium Bicarbonate 1 mEq/kg IV/IO if suspected hyperkalemia (e.g. dialysis patient) or tricyclic antidepressant OD (max 50mEq)
- Double Sequential Defibrillation
- Indications (all must be met):
- Refractory Ventricular Fibrillation/Pulseless Ventricular Tachycardia (persistent ventricular fibrillation/pulseless ventricular tachycardia without any transient interruption of ventricular fibrillation/ventricular tachycardia, not converted by standard defibrillation of 5 shocks or more)
- H & T’s addressed (if applicable)
- 450mg of Amiodarone administered and failed
- Procedure:
- Emphasis on minimizing interruptions in compressions
- Apply an additional set of pads (anterior/posterior)
- Verify that both monitors are attached and confirm Ventricular Fibrillation/pulseless ventricular tachycardia
- Charge both monitors to maximum energy setting and ensure all team members are clear of the patient
- Defibrillate by pressing both shock buttons as synchronously as possible
- Follow defibrillation with immediate compressions
- Indications (all must be met):
Contact Medical Control for Additional Orders if Needed
Cardiac Arrest - Post Resuscitation Care
Basic Life Support
- Maintain assisted ventilation as needed
- Obtain blood glucose level
- Supplemental 100% oxygen
- Including ETCO2 level (35-45 normal)
Advanced Life Support
- Full ALS Assessment and Treatment
- Obtain a 12 lead ECG and initiate STEMI Alert if criteria exists
- For hypotension (systolic BP < 90 mmHg) not improved by fluid boluses, or when fluid boluses are contraindicated
- Norepinephrine infusion at 0.5-16 mcg/minute IV/IO if available; otherwise use push dose pressors titrated to SBP>90 mm Hg or max dose (10ml) reached.
- Start infusion at around 8-12 mcg/minute (30-45 gtt/min), titrated to maintain SBP > 90 mm Hg (see pg. 10-27 for infusion preparation chart)
- Administer supplemental oxygen with a target oxygen saturation of 94-98%
- For patients with assisted ventilation, provide 10-12 breaths per minute with a target ETCO2 of 35-40 mmHg
- Treat arrhythmias as directed by appropriate Cardiac Arrhythmias protocol
- No additional anti-arrhythmic is required unless arrhythmia reoccurs
- If cardiac arrest reoccurs refer to appropriate algorithm based on presenting rhythm:
- Total cumulative dose of Amiodarone should not exceed 450 mg (300mg + 150 mg)
- If patient becomes combative, administer Midazolam (Versed) 2.5 mg slow IV or 5 mg IM or intranasal via MAD
- Repeat Midazolam (Versed) 2.5 mg slow IV or 5 mg IM or intranasal via MAD if patient still combative
- Transport to the nearest PCI (Percutaneous Coronary Intervention) capable hospital
- PCI capable hospital campuses in and around Osceola County:
- Osceola Regional Medical Center
- P. Phillips Hospital
- Holmes Regional Medical Center
- Heart of Florida Regional Medical Center
- Lawnwood Regional Medical Center
- Southlake Hospital
- Advent Health Celebration
- Indian River Medical Center
- PCI capable hospital campuses in and around Osceola County:
Contact Medical Control for Additional Orders if Needed
Cardiac Arrest – Termination of Resuscitation Medical
The paramedic has the discretion to continue resuscitation efforts in any case despite Termination of Resuscitation criteria being met if scene safety, location, patient’s age, time of arrest, or bystander input compels this decision. When asystole is seen on the cardiac monitor confirmation of the rhythm shall include a printed rhythm strip, as well as interpretation of the rhythm in more than one lead. Low amplitude V-Fib or PEA may be difficult to distinguish from asystole when using only the cardiac monitor display for interpretation.
Medical Control Contact Not Required
The paramedic may terminate resuscitative efforts in nonhypothermic adults provided all 5 of the following criteria exist:
- Initial rhythm is asystole and remains asystolic throughout, confirmed in two leads and on printed rhythm strip
- Secure airway confirmed by digital capnography (ETT or SGA)
- At least four doses of Epinephrine have been administered (given every 3-5 min)
- Cardiac arrest refractory for at least 20 minutes of ACLS
- Quantitative ETCO2 value is < 10 mmHg with effective CPR, after 20 minutes of ACLS
Contact Medical Control for any extenuating circumstances and provide the following information
- Initial rhythm and terminal rhythm
- Method of airway management and vascular access
- Medications given during the arrest
- ETCO2 value
- Total amount of time working the arrest
*Do not terminate resuscitation if transport has been initiated*
Contact Medical Control for Additional Orders if Needed
Cardiac Arrest – No Resuscitation Attempt
No resuscitation attempt is indicated for cardiac arrest in the following scenarios:
Obvious signs of death:
- Pulseless, apneic and no other signs of life present AND any of the following:
- Diffuse signs of rigor mortis
- Diffuse signs of decomposition of body tissues
- Dependent lividity
- Injuries incompatible with life (e.g. incineration, decapitation, hemicorporectomy)
- Document the obvious signs of death as listed above in report
Blunt or penetrating trauma (all criteria must be met):
- Pulseless, apneic and no other signs of life present
- Lack of pupillary reflexes and spontaneous movement
- Asystole on cardiac monitor
Patients who become pulseless after severe traumatic injury when transport to the nearest ED cannot be initiated within 15 minutes (i.e. prolonged extrications) provided that all other signs of life are absent and transport has not been initiated, contact Medical Control
"Do Not Resuscitate" (DNR Order)
- When presented with a valid and complete State of Florida DO NOT RESUSCITATE order (Form 1896)
- Must be on YELLOW Paper and signed by the patient's physician
Other Circumstances
Use caution in termination of resuscitation in the following scenarios:
- When mechanism of injury is inconsistent with traumatic cardiac arrest
- Lightning or other high voltage electrical injuries
- Drowning
- Suspected hypothermia
- Consider Contacting medical control for the above situations
In order to preserve trace evidence at a death scene, avoid covering the body when it is prudent and reasonable to do so. In the scenario when a person is deceased at a residence or other private area, partition off, or otherwise restrict access to, the area where the body is as opposed to covering the body. Law Enforcement Officers on the scene should be involved in the decision to how best respect the patients dignity without compromising investigative needs.
There is no strict contraindication on covering the deceased, especially when the crews are trying to protect the dignity of the deceased or the mental state of their family.
Contact Medical Control for Additional Orders if Needed
Cardiac Arrhythmias – Atrial Fibrillation/Flutter
Atrial Fibrillation or Flutter – Heart Rate over 150
Basic Life Support
- Supplemental oxygen
- Including ETCO2 level (35-45 normal)
Advanced Life Support
- Full ALS Assessment and Treatment
- Do not delay treatment if patient is unstable by obtaining 12 lead ECG unless diagnosis is in question
Borderline or stable systolic blood pressure > 90 mmHg:
- Rate < 150 beats/min
- No anti-arrhythmic indicated
- Provide supportive care and expedite transport
- Rate ≥ 150 beats/min AND symptomatic (chest pain, palpitations, dyspnea)
- Administer Diltiazem (Cardizem) 10mg over two minutes if available
(initial dosage) - Administer second dosage of Diltiazem (Cardizem) 10mg after 5- 10 minutes if no rate change (20mg max dosage)
- If BP < 90 mm Hg systolic, administer boluses of 0.9% NaCl at 250 ml until systolic BP > 90 mm Hg
- Contraindicated if bp <90
- Contraindicated if wide complex (QRS > 120 msec) or history of Wolf-Parkinson- White (WPW) syndrome
- Unstable with serious signs and symptoms (Ventricular rate > 150):
- Administer Diltiazem (Cardizem) 10mg over two minutes if available
- Unstable is defined as systolic blood pressure less than 90 mmHg, acutely altered mental status, or signs of shock
- Synchronized cardioversion; some patients may require sedation prior to cardioversion. Ketamine 0.5mg/kg IV (50mg max) can be used
- 1st energy level 100 Joules
- If no response 200 J
- If no response 300 J
- If no response 360 J
Contact Medical Control for Additional Orders if Needed
Bradycardia (Heart Rate less than 50)
Basic Life Support
- Supplemental oxygen
- Including ETCO2 level (35-45 normal)
Advanced Life Support
- Full ALS Assessment and Treatment
- Administer boluses of 0.9% NaCl at 250 ml until systolic BP > 90 mm Hg
- Contraindicated if evidence of congestive heart failure (e.g. rales)
- Do not delay treatment if patient is unstable by obtaining 12 lead ECG unless diagnosis is in question
- If the patient is normotensive, with no signs of shock, provide supportive care and expedite transport
Unstable Bradycardia with serious signs and symptoms (Heart rate < 50):
- Unstable is defined as systolic blood pressure less than 90 mmHg or acutely altered mental status.
- If IV establish, administer Atropine 1 mg IV
- Repeat every 3 minutes as needed (Maximum 3 mg)
- If symptoms persist after Atropine, or any delay in establishing IV, initiate transcutaneous pacing using Demand Mode:
- Start at lowest milliamps; increase until electrical capture with pulses achieved
- Start rate at 70 or default and increase rate to achieve systolic BP ≥ 90 mm Hg (Maximum 100 beats/minute)
- If systolic BP returns to > 90 mmHg consider sedation, Midazolam 2.5 mg slow IV or Ketamine 0.5mg/kg IV (50mg max)
- For symptomatic unstable bradycardia not improved by the above:
- Epinephrine infusion at 2-10 mcg/minute IV/IO, titrated to BP and HR with improved clinical status of patient. (see infusion preparation chart)
- For symptomatic unstable bradycardia not improved by the above:
- Norepinephrine infusion at 0.5-16 mcg/minute IV/IO, titrated to maintain SBP > 90 mm Hg (see pg. 10-27 for infusion preparation chart) OR
- Push dose epinephrine: Remove 9ml (0.9mg) of 1:10,000 Epinephrine from the pre-filled syringe then draw 9ml of NS into the pre-filled syringe and mix solution. Concentration 10mcg/ml. IV push 1ml every minute to increase blood pressure to 90 mmHg and heart rate to 50; max 10ml (100mcg).
- If above unsuccessful:
- Epinephrine infusion at 2-10 mcg/minute IV/IO, titrated to BP and HR with improved clinical status of patient. (see pg. 10-14 for infusion preparation chart)
- If drug induced, treat for specific drug overdose:
- Beta Blocker/Calcium Channel Blocker OD
- Administer Calcium Chloride 1 gram IV/IO (should pretreat with Zofran-see protocol)
- Contraindicated if patient on Digoxin / Lanoxin
- Administer Glucagon 1mg IV/IO/IM/IN (should pretreat with Zofran-see protocol)
- Opioid OD
- Administer Naloxone (Narcan) 2 mg IV (start at 0.4 mg for patients over 65 years old)
- Naloxone (Narcan) can be given in 0.4 mg increments titrated to mental status and respiratory drive
- If IV access has not been established, give IM or via Mucosal Atomizer Device (MAD)
- Tricyclic Antidepressant OD
- Administer Sodium Bicarbonate 1 mEq/kg IV (max 50 mEq)
Contact Medical Control for Additional Orders if Needed
Supraventricular Tachycardia
Basic Life Support
- Supplemental oxygen
- Including ETCO2 level (35-45 normal)
Advanced Life Support
- Full ALS Assessment and Treatment
- Do not delay treatment if patient is unstable by obtaining 12 lead ECG unless diagnosis is in question
Stable or borderline (Ventricular rate > 150):
- Vagal maneuvers (Valsalva or cough)
- Ice water contraindicated in patients with ischemic heart disease
- Vagal maneuvers shall be accompanied by passive leg elevation of the patient
- Adenosine Phosphate (Adenocard) 6 mg rapid IV over 1-3 seconds
- If no response in 2 minutes, 12 mg rapid IV over 1-3 seconds
Unstable with serious signs and symptoms (Ventricular rate > 150):
- Unstable is defined as systolic blood pressure less than 90 mmHg, acutely altered mental status, or signs of shock
- May give brief trial of Adenosine 6mg rapid IV over 1-3 seconds
- Synchronized Cardioversion; some patients may require sedation prior to cardioversion. Ketamine 0.5mg/kg IV (50mg max) can be used
- 1st energy level 100 Joules
- If no response 200 J
- If no response 300 J
- If no response 360 J
Cardiac Arrhythmias – Wide Complex Tachycardia
Basic Life Support
- Supplemental oxygen
- Including ETCO2 level (35-45 normal)
Advanced Life Support
- Full ALS Assessment and Treatment
- Do not delay treatment if patient is unstable by obtaining 12 lead ECG unless diagnosis is in question
- In general, assume unknown wide complex tachycardias, at rates over 150, represent ventricular tachycardia
Stable and SVT highly likely (rate > 150):
- Adenosine Phosphate (Adenocard) 6 mg rapid IV over 1-3 seconds
- If no response in 2 minutes, 12 mg rapid IV over 1-3 seconds
Stable wide complex or ventricular tachycardia likely (rate > 150):
- Amiodarone 150 mg IV Piggyback over 10 minutes
- Repeat Amiodarone 150 mg IV Piggyback over 10 minutes every 10-15 minutes (Maximum of 450 mg total)
- Or consider Lidocaine
- Lidocaine IV/IO initial dose: 1–1.5 mg/kg
- If persistent VT then Lidocaine IV/IO repeat dose: 0.5–0.75 mg/kg every 5 to 10-minutes with maximum cumulative dose of 3 mg/kg
- Lidocaine IV/IO initial dose: 1–1.5 mg/kg
Unstable wide complex tachycardia (rate > 150):
- Unstable is defined as systolic blood pressure less than 90 mmHg, acutely altered mental status, or signs of shock
- Synchronized cardioversion
- 1st energy level 100 Joules
- If no response 200 J
- If no response 300 J
- If no response 360 J
- If delays in synchronization occur and clinical condition is critical, go immediately to unsynchronized shocks
- If wide complex tachycardia re-occurs following electrical cardioversion:
- Amiodarone 150 mg IV Piggyback over 10 minutes
- Repeat Amiodarone 150 mg IV Piggyback over 10 minutes every 10-15 minutes (Maximum of 450 mg total)
- Or consider Lidocaine
- Lidocaine IV/IO initial dose: 1–1.5 mg/kg
- If persistent VF/VT then Lidocaine IV/IO repeat dose: 0.5–0.75 mg/kg every 5 to 10-minutes with maximum cumulative dose of 3 mg/kg
- Lidocaine IV/IO initial dose: 1–1.5 mg/kg
- Amiodarone 150 mg IV Piggyback over 10 minutes
- If hyperkalemia suspected in any wide complex tachycardia (e.g. renal failure patient) administer the following medications:
- Calcium Chloride 1 gram IV
- Contraindicated if patient on Digoxin/Lanoxin
- Sodium Bicarbonate 1 mEq/kg IV (max 50 mEq)
- Calcium Chloride 1 gram IV
Contact Medical Control for Additional Orders if Needed
Cardiac Arrhythmias – Polymorphous VT (Torsades)
Basic Life Support
- Supplemental oxygen
- Including ETCO2 level (35-45 normal)
Advanced Life Support
- Full ALS Assessment and Treatment
- Do not delay treatment by obtaining ECG unless diagnosis is in question
Stable:
- Magnesium Sulfate 2 g slow IV in 10 ml NS over 1-2 minutes
- If no response, Amiodarone 150 mg IV Piggyback over 10 minutes
- Repeat Amiodarone 150 mg IV Piggyback over 10 minutes every 10-15 minutes (Maximum of 450 mg total)
- Or consider Lidocaine
- Lidocaine IV/IO initial dose: 1–1.5 mg/kg
- If persistent VF/VT then Lidocaine IV/IO repeat dose: 0.5–0.75 mg/kg every 5 to 10-minutes with maximum cumulative dose of 3 mg/kg
- Follow with continuous infusion of 1 to 4 mg/minute after return of perfusion
- Lidocaine IV/IO initial dose: 1–1.5 mg/kg
Note: closely monitor vital signs as both Magnesium Sulfate and Amiodarone cause hypotension
Unstable – or if no response to the above measures:
- Unstable is defined as systolic blood pressure less than 90 mmHg and acutely altered mental status, or signs of shock.
- Unsynchronized Cardioversion
- 1st energy level 100 Joules
- If no response 200 J
- If no response 300 J
- If no response 360 J
Contact Medical Control for Additional Orders if Needed
Chest Pain – Suspected Cardiac Ischemia
Basic Life Support
- Supplemental oxygen
- Including ETCO2 level (35-45 normal)
- Assist patient in self-administration of previously prescribed Aspirin
- Assist patient in self-administration of previously prescribed Nitroglycerin
- Contraindicated if systolic BP < 90 mm Hg
- Contraindicated if use of a Phosphodiesterase-5 (PDE5) inhibitor within last 24 hours (Viagra or Levitra); 48 hours for Cialis
- Repeat patient assisted Nitroglycerin administration every 5 minutes as needed for continued chest pain (provided SBP remains > 90 mm Hg) with assessment of patient before and after each NTG dose
Advanced Life Support
- Full ALS Assessment and Treatment
- Perform 12 lead ECG immediately (within 3 mins unless extreme circumstances):
- Identify the presence of ECG changes suggestive of Acute Myocardial Infarct (AMI)
- Perform 2nd EKG once patient is loaded in rescue
- Perform 3rd EKG 3 minutes prior to arrival at receiving facility
- If STEMI criteria are present initiate STEMI Alert (see following page)
- Aspirin 324 mg PO, chewed if patient is able to swallow
- Known allergy to Aspirin (clarify allergy)
- Aspirin is NOT contraindicated if ACS (Acute Coronary Syndrome) suspected and taking Warfarin (Coumadin) or other anticoagulant or antiplatelet, unless active bleeding
- Document reason Aspirin not administered (if aspirin taken > 6 hours prior to EMS arrival, aspirin should be administered)
- Nitroglycerin 0.4 mg spray or tablet SL, every 5 minutes as needed for chest pain
- IV access should be established prior to Nitroglycerin administration
- Contraindicated if systolic BP < 90 mm Hg
- Contraindicated if use of a Phosphodiesterase-5 (PDE5) inhibitor within last 24 hours (Viagra or Levitra); 48 hours for Cialis
- Contraindicated in Acute Inferior Wall MI or Right Ventricular Infarct unless discussed with and approved by on-line Medical Control
- Be prepared to administer NS 250 ml boluses IV if hypotension develops
- Fentanyl (Sublimaze) 1 mcg/kg (maximum 100 mcg) slow IV; repeat once after 5 minutes as needed OR 100 mcg intranasal via MAD (divide dose equally between each nare). Maximum cumulative dose is 200 mcg; this is if no chest pain relief after 3rd Nitroglycerin dose
- Contraindicated if systolic BP < 100 mm Hg
- Use with caution if right ventricular or posterior wall MI (ST elevation in posterior leads with marked depression V1 thru V4)
- If runs of Ventricular Tachycardia (4 beats or greater) occur:
- Amiodarone 150 mg IV Piggyback over 10 minutes OR
- Lidocaine IV/IO initial dose: 1–1.5 mg/kg
- If persistent VF/VT then Lidocaine IV/IO repeat dose: 0.5–0.75 mg/kg every 5 to 10-minutes with maximum cumulative dose of 3 mg/kg
- Follow with continuous infusion of 1 to 4 mg/minute
- If persistent VF/VT then Lidocaine IV/IO repeat dose: 0.5–0.75 mg/kg every 5 to 10-minutes with maximum cumulative dose of 3 mg/kg
- Isolated PVC’s do not require treatment
- For patients with severe nausea or vomiting:
- Ondansetron (Zofran), 4mg slow IV or 4 mg Oral Disintegrating Tablet (ODT) by mouth
STEMI Alert (ST Elevation Myocardial Infarction)
A STEMI Alert will be instituted for patients having chest pain or ischemic equivalent symptoms for < 12 hours, and any of the following:
- ST segment elevation ≥ 1mm in two or more contiguous leads
- Computer interpretation of “Meets ST Elevation MI criteria” or similar wording on 12 lead ECG
Accomplish the following as part of the STEMI Alert process:
- Follow chest pain protocol
- Determine if the patient has a Cardiologist
- Transmit the 12 lead ECG to the appropriate hospital destination
- During the radio call to the ED, convey the name of the patient's Cardiologist
- Transport STEMI Alert patients to a PCI (Percutaneous Coronary Intervention) capable hospital, if ground transport expected to take 20 minutes or greater consider air transport
- PCI capable hospital campuses in and around Osceola County:
- Osceola Regional Medical Center
- Orlando Regional Medical Center
- Advent Health Hospital Orlando
- Advent Health Celebration
- P. Phillips Hospital
- Holmes Regional Medical Center
- Heart of Florida Regional Medical Center
- Lawnwood Medical Center
- Southlake Hospital
- Indian River Medical Center
- PCI capable hospital campuses in and around Osceola County:
Contact Medical Control for Additional Orders if Needed
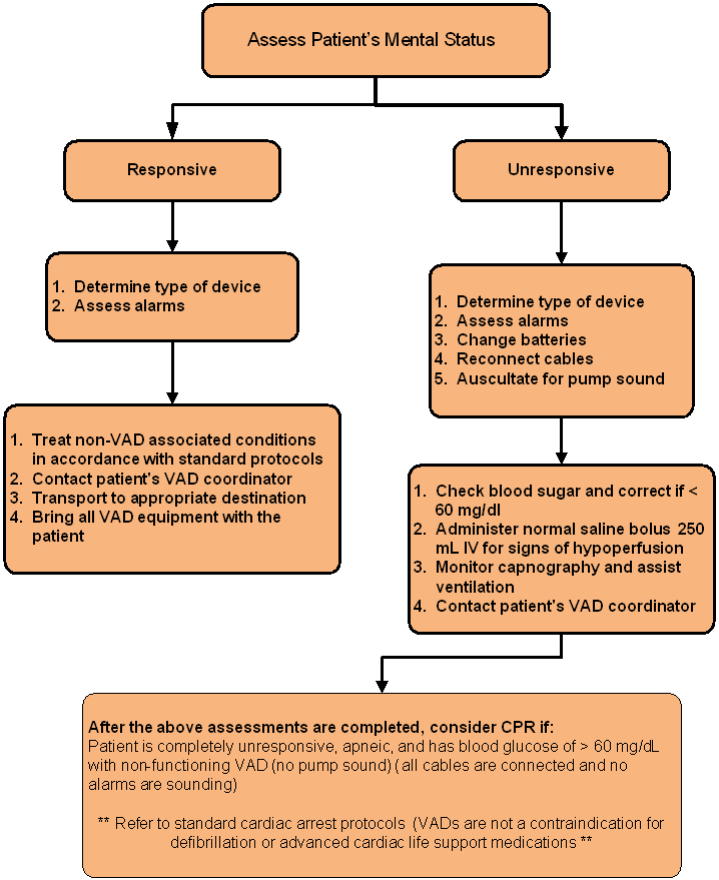
Ventricular-Assist Devices - VADs
General Approach to Patients with VADs
Ventricular-Assist Devices (VADs) are surgically implanted circulatory support devices designed to assist the pumping action of the heart. Caring for these patients is complicated, and every effort should be made to contact the patient’s primary caretaker (spouse, guardian, etc) and VAD coordinator during your evaluation. Patients with properly functioning VADs may not have a detectable pulse, normal blood pressure or oxygen saturation.
- Treat non-VAD associated conditions in accordance with the appropriate Osceola County EMS System protocol
- If patient meets Trauma or Stroke Alert criteria, transport them to the appropriate receiving facility
- If a patient meets STEMI Alert criteria, transport them to a PCI capable VAD Center
- Contact the patient's VAD coordinator immediately (if patient or caretaker does not have this information, look on the device for a phone number)
- For any condition that is suspected to be related to the LVAD, transport to the patient's requested VAD Center Contact Medical Control upon initiation of medical care
- Always bring all available VAD equipment to the Emergency Department with the transported patient
Basic Life Support
- Establish patent airway
- Supplemental 100% oxygen
- Including ETCO2 level (35-45 normal)
- Record blood glucose level if any weakness, altered mental status or history of diabetes
- Assist patient in replacing the device's batteries or cables
Advanced Life Support
- Full ALS Assessment and Treatment
- Monitor capnography to assess ventilation and perfusion
- Administer boluses of 0.9% NaCl at 250 ml if signs of hypoperfusion (MAP < 60)
- Evaluate unresponsive patients carefully (listen for device in chest, CPR is contraindicated if device can be heard) chest compressions may cause irreversible damage to devices and catastrophic internal hemorrhage to the patient.
- Mechanical CPR devices are contraindicated in VAD patients
- Evaluate for reversible causes prior to initiation of CPR, and treat according to cardiac arrest protocols.
- Expedite transport and treat other conditions as per appropriate protocols