
Pediatric Medical
General Approach
Airway Emergencies
Confirmation of Advanced Airway Placement
Allergic Reactions
Altered Mental Status
Apparent Life Threatening Event (ALTE) Brief Resolved Unexplained Event (BRUE)
Drowning
Dyspnea
Foreign Body Airway Obstruction
Overdose, Poisoning, or Ingestion
Pain Management
Seizures
Transport of Pediatric Patients
General Approach to All Pediatric Patients
The following measures will apply to the management of all pediatric patients:
- A Child shall be defined as:
- Age ≤ 18 years or weight ≤ 40 kilograms (if age unknown)
- For PALS resuscitation: infant up to puberty
- For Trauma alert: 15 years or less
Basic Life Support
- Establish patient responsiveness
- Immobilize spine if cervical or other spine injury suspected
- Assess airway and breathing
- Supplemental 100% oxygen if any respiratory signs or symptoms
- Assess circulation and perfusion by measuring heart rate, and observing skin color, temperature, capillary refill, and the quality of central/peripheral pulses
- For children with absent pulses initiate cardiopulmonary resuscitation
- Control active bleeding with direct pressure, hemostatic gauze packing and/or tourniquet, as indicated
- Measure BP in children older than 3 years of age
- Evaluate mental status, including pupil reaction, motor function and sensation
- For mental status, use the AVPU scale:
- A- The is patient alert and oriented (age appropriate)
- V- The patient is responsive to verbal stimulus
- P- The patient is responsive to painful stimulus
- U- The patient is unresponsive to any stimulus
- For mental status, use the AVPU scale:
- Expose the child only as necessary to perform further assessments
- Maintain the child’s body temperature throughout the examination
Advanced Life Support
- When condition warrants (specified as “Full Pediatric ALS Assessment and Treatment” in individual protocols):
- Advanced airway/ventilatory management as needed
- Perform cardiac monitoring
- Continuously monitor oxygen saturation and capnography
- If symptoms severe or for medication access IV 0.9% NaCl KVO or IV lock
- If signs of shock administer boluses of 0.9% NaCl at 20ml/kg and re-assess until signs of shock resolve or 60ml/kg total; if still hypotensive despite 60ml/kg, start vasopressors
- If signs of severe cardiopulmonary compromise and IV attempts unsuccessful, establish intraosseous access
- If child’s condition is critical or unstable, initiate transport without delay
- For patients with severe nausea or vomiting:
- Ondansetron (Zofran), 2 mg (8-15 kg) or 4 mg (>15 kg) oral disintegrating tablet (ODT) by mouth (break 4 mg tablet in half for 2 mg dose)
- Use HandTevy guide to determine medication dosages and equipment sizes
- Reassess the patient frequently (vital signs every 5 minutes)
Airway Emergencies
Basic Life Support
- If suspicion of trauma, maintain C-spine immobilization
- Suction all debris, secretions from airway
- Bag valve mask with OPA/NPA ventilate; use only sufficient volume and force to just make chest rise visibly
- Ventilate at a rate of 12-20 breaths/minute, using the higher rate for younger ages
- Supplemental 100% oxygen
- Including ETCO2 level (35-45 normal)
Advanced Life Support
- Have assistant apply cardiac monitor as soon as possible
- Address cardiac rhythm abnormalities per appropriate protocol
- Monitor end-tidal CO2 and oxygen saturation continuously
- BVM ventilate at least 2 minutes with 100% oxygen to achieve O2 saturation >90%
- Follow sequence listed below (use Medical Director approved device to select appropriate equipment)
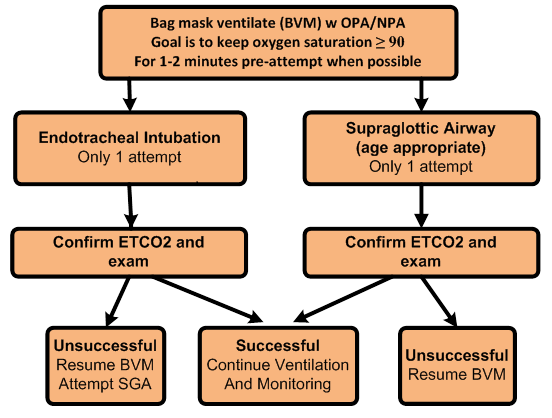
- At every step of airway algorithm, effective bag valve mask ventilation is an acceptable level of airway management and often preferable in pediatric patients
- Components of effective ventilation include oxygenation, chest rise and fall, adequate lung sounds, and the presence of an alveolar waveform on capnography
- Monitor ETCO2, oxygen saturation and assess for effective ventilation continuously
Contact Medical Control for Additional Orders if Needed
Confirmation of Advanced Airway Placement and Effectiveness of Ventilation
Capnography/ETCO2 Monitoring:
- Digital capnography (waveform) is the system standard for ETCO2 monitoring and continuous ETCO2 monitoring is a mandatory component in the management of critical patients and invasive airway management
- Immediately after placing an ETT or SGA capnography shall be re-applied to confirm proper placement
- Proper placement is indicated by the presence of a continuous alveolar waveform on
- If an alveolar waveform is not initially present, or disappears after 3-5 breaths (i.e. flat-line), remove the ETT or SGA and proceed to the next step in the algorithm
- If ETCO2 monitoring cannot be accomplished by the above method, the invasive airway device must be removed, and the airway managed noninvasively
Additional Measures
- Assess epigastric sounds, breath sounds, and chest rise and fall
- Record tube depth and secure in place using a commercial tube holder
- Utilize head restraint devices or rigid cervical collar and long spine board immobilization as needed to help secure airway device in place
Allergic Reactions
Basic Life Support
- Assist patient in self-administration of previously prescribed epinephrine (Epi-Pen)
- Nothing by mouth
Advanced Life Support
- If Moderate or Severe symptoms, perform Full Pediatric ALS Assessment and Treatment
Mild Reaction (Itching/Hives)
- Diphenhydramine (Benadryl) 1 mg/kg IV (Maximum 50 mg)
- May be administered IM if no IV access available
Moderation Reaction (Dyspnea, Wheezing, Chest tightness)
- Albuterol (Proventil) 2.5 mg/3 ml via and Ipratropium Bromide 0.02% (Atrovent) 0.5 mg/2.5 ml via nebulizer
- Repeat Albuterol (Proventil)/Ipratropium Bromide (Atrovent) X 2 for continued wheezing
- Diphenhydramine (Benadryl) 1 mg/kg IV/IO (Maximum 50 mg)
- May be administered IM if no IV access available
- Methylprednisolone (Solumedrol) 2 mg/kg IV or IM (Maximum individual dose 125 mg)
Severe Reaction (anaphylactic shock, stridor, severe respiratory distress, lip or tongue swelling; or if patient has hives/itching PLUS dyspnea, wheezing or chest tightness; or hives/itching or dyspnea/wheezing PLUS vomiting or abdominal pain (with likely allergen for that patient )
- Epinephrine 1:1,000 solution 0.01mg/kg IM (max dose 0.3mg)
- Massage injection site vigorously for 30-60 seconds
- Repeat Epinephrine in 3 minutes if signs of severe reaction or shock persist after initial dose
- If anaphylactic shock (signs of shock + hypotensive for age despite 60ml/kg of fluid and two doses of IM 1:1000 epinephrine), start an Epinephrine drip
- Albuterol (Proventil) 2.5 mg/3 ml and Ipratropium Bromide 0.02% (Atrovent) 0.5 mg/2.5 ml via nebulizer
- Repeat Albuterol (Proventil)/Ipratropium Bromide (Atrovent) X 2 for continued wheezing
- Diphenhydramine (Benadryl) 1 mg/kg IV/IO (Maximum 50 mg)
- May be administered IM if no IV access available
- Methylprednisolone (Solumedrol) 2 mg/kg IV or IM (Maximum individual dose 125 mg)
Contact Medical Control for Additional Orders if Needed
Altered Mental Status
Basic Life Support
- If trauma suspected, stabilize spine
- Supplemental 100% oxygen
- Including ETCO2 level (35-45 normal)
- Blood glucose check
Advanced Life Support
- Full Pediatric ALS Assessment and Treatment
- Determine blood glucose and treat glucose < 70 mg/dl
- Dextrose 10% 0.2gm/kg (max12.5gm) (Follow HandTevy Guide)
- If no IV available:
- Glucose paste or other oral glucose containing agent (e.g. orange juice) if patient alert enough to self administer oral agent
- Glucagon 0.5mg - 1mg IM/IN (Follow HandTevy Guide)
- If hypoglycemia persists:
- Repeat blood glucose check
- Repeat Dextrose (as above) once if blood glucose < 70 mg/dl after 10 minutes
- Naloxone at 0.1 mg/kg (Maximum individual dose 2.0 mg) via mucosal atomizer device (MAD), IV, IM or IO route
NOTE: Pediatric patients that have been administered medication, shall be transported to the appropriate receiving facility. If medications have been administered and parent/guardian refuses transport, contact Medical Control immediately.
Contact Medical Control for Additional Orders if Needed
Apparent Life Threatening Event (ALTE)
Brief Resolved Unexplained Event (BRUE)
Brief Resolved Unexplained Event (BRUE) formerly known as Apparent Life Threatening Event (ALTE) is an episode that is frightening to the observer, and involves some combination of the below. BRUE is replacing ALTE in Pediatrics and Emergency Medicine but requires a full history and exam by a clinician to determine that no other likely explanation is the cause of the event. Either term is acceptable.
BRUE: Brief Resolved Unexplained Event that was observed by caregiver in a child less than one year of age, and no obvious explanation for event identified (eg., hx of Tetralogy of Fallot);
- Absent, decreased or irregular breathing
- Cyanosis or pallor
- Marked change in muscle tone (hyper or hypotonia)
- Altered responsiveness
ALTE is less well defined, but term is still in use for Acute Life Threatening Event
History of a BRUE/ALTE may represent serious illness, even if the infant appears entirely well by the time he or she is evaluated. The apparent well-being should not be considered evidence that a potentially life-threatening event with successful resuscitation did not occur if the clinical history indicates otherwise.
Basic Life Support
- Assume the history given is accurate and reliable
- Determine the severity, nature and duration of the episode
- Obtain a medical history:
- Known chronic diseases
- History of preterm delivery
- Evidence of seizure activity
- Current or recent infections
- Gastroesophageal reflux
- Inappropriate mixture of formula
- Recent trauma
- Perform a thorough physical assessment that includes the general appearance, skin color, level of interaction with environment, and evidence of trauma
- Transport to the nearest appropriate receiving facility
- Contact with Medical Control is required prior to accepting a refusal for patients ≤ 12 months of age
- If necessary contact Law Enforcement to ensure transport of the child
Contact Medical Control for Additional Orders if Needed
Drowning – Pediatric
Basic Life Support
- Spinal immobilization if pool related event or circumstances uncertain
- Protect from heat loss
- Supplemental 100% oxygen
- Including ETCO2 level (35-45 normal)
- may need to utilize airway adjuncts like an NPA
Advanced Life Support
- Perform Full Pediatric ALS Assessment and Treatment
- Patients may develop delayed onset respiratory symptoms
- Consider CPAP (10cm H2) for patients with significant dyspnea or hypoxia if size allows
- Contraindications: decreased LOC, lack of spontaneous respirations, SBP <90 mm Hg
- You may also consider high flow oxygen at 1-2 liters/kg via the Nasal Cannula added ot the Non-rebreather for dyspnea or hypoxia
- Consider CPAP (10cm H2) for patients with significant dyspnea or hypoxia if size allows
- If hypotensive and lungs are clear, administer 20cc/kg of fluids. If hypotensive and signs of fluid overload (crackles, wheezing), start vasopressors.
- Refer to appropriate protocol if cardiac arrest present
- Transport drownings to the nearest Pediatric hospital (Advent Celebration, Arnold Palmer Hospital for Children or Nemours Children's Hospital) unless signs of trauma or diving injury, then transport to the nearest state approved Pediatric trauma center. Arnold Palmer and Nemours have ECMO capability.
- Trauma Alert only if peds trauma alert criteria met, then transport to the nearest State Approved Pediatric Trauma Center
Note: If parents are refusing transport after a submersion injury, medical control contact is required prior to accepting refusal.
Dyspnea
Basic Life Support
- Supplemental 100% oxygen
- Including ETCO2 level (35-45 normal)
- If foreign body obstruction is suspected refer to foreign body protocol
Advanced Life Support
- Full Pediatric ALS Assessment and Treatment
- For bronchospasm:
- Albuterol (Proventil) 2.5mg/3ml and Ipratropium Bromide 0.02% (Atrovent) 0.5mg/2.5ml via nebulizer over 10-15 minutes
- Repeat Albuterol (Proventil)/Ipratropium Bromide (Atrovent) X 2 for continued wheezing
- Methylprednisolone (Solumedrol) 2 mg/kg IV or IM (Maximum individual dose 125
- If patient shows signs of worsening respiratory distress, inadequate ventilation or respiratory failure in the setting of bronchospasm or a history of asthma:
- Epinephrine 1:1,000 at 0.01 mg/kg (max 0.3 mg) IM
- May repeat Epinephrine every 15 minutes X 2 additional doses (3 total) if severe symptoms persist
- May administer at same time nebulizer is being administered
- Epinephrine 1:1,000 at 0.01 mg/kg (max 0.3 mg) IM
- Magnesium Sulfate 50 mg/kg IV over 5-10 minutes; contraindicated if history of renal failure
- Albuterol (Proventil) 2.5mg/3ml and Ipratropium Bromide 0.02% (Atrovent) 0.5mg/2.5ml via nebulizer over 10-15 minutes
- If partial upper airway obstruction or stridor without severe respiratory distress:
- Do nothing to upset the child
- Perform critical assessments only
- Have parent administer blow by supplemental oxygen
- Place patient in position of comfort
- Do not obtain vascular access
- Expedite transport
- If complete airway obstruction, or severe respiratory distress, failure, or arrest
- Advanced airway/ventilatory management as needed
Contact Medical Control for Additional Orders if Needed
Foreign Body Airway Obstruction
- If unresponsive, open airway using a head tilt/chin lift (if no trauma)
- If < 1 year old, administer up to 5 back blows and 5 chest compressions
- If ≥ 1 to 8 years, administer abdominal thrusts until foreign body dislodged
- If ventilation is unsuccessful (O2 saturations cannot be kept > 90) perform the following in order:
- Reposition airway and attempt bag valve mask assisted ventilation again
- If unsuccessful, establish direct view of object and attempt to remove it with Magill forceps
- If unable to visualize a foreign body using laryngoscope, and vocal cords are clearly seen, attempt intubation only once
- If unsuccessful, re-attempt BVM ventilation; if oxygen saturation > 90, and good end tidal wave form continue ventilation with BVM and expedite transport
- If patient cannot be ventilated/oxygenated with the above measures, contact Medical Control to consider need cricothyrotomy (patients < 8 years of age)
- If complete obstruction below the vocal cords and FB not removable, then intubate into right mainstem bronchus to advance FB with ETT, then pull back ETT and ventilate left lung.
- Expedite transport to nearest emergency department
Overdose, Poisoning, or Ingestion – Pediatric
For any overdose or poisoning contact should be made with the Regional Poison Control Center (800-222-1222). Whenever possible, determine the agent(s) involved, the time of the ingestion/exposure, and the amount ingested. Bring empty pill bottles, etc., to the receiving facility.
Advanced Life Support
- If any symptoms present perform Full Pediatric ALS Assessment and Treatment
- If respiratory depression is present and an overdose is suspected:
- Naloxone at 0.1 mg/kg (Maximum dose 2.0 mg) via MAD, IV, IO, or IM route
Treatment for specific toxic exposures is indicated only when patients are clearly symptomatic. In the absence of significant symptoms, monitor closely and expedite transport. If indicated initiate HAZMAT alert.
Organophosphates
Symptoms include dyspnea, bronchorrhea, lacrimation, vomiting/diarrhea, weakness, paralysis, seizures
- Atropine 0.02 mg/kg IV (minimum dose 0.1 mg)
- If seizures present see Pediatric Seizure Protocol
Tricyclic Antidepressant
Symptoms include hypotension, arrhythmias, wide QRS complex (>0.09 sec)
- Sodium Bicarbonate (Follow HandTevy Guide for concentrations and dosages)
Calcium Channel Blockers and Beta Blockers
Symptoms include bradycardia, hypotension and heart blocks
- Glucagon 0.5-1.0 mg/kg IM/IN (Maximum dose 1.0 mg)
- If symptoms persist, Atropine 0.02 mg/kg (minimum dose 0.1 mg)
- If poisoning due to a calcium channel blocker, Calcium Chloride 0.2 ml/kg slow IV (Max 2g)
Dystonic Reaction
Acute uncontrollable muscle contractions
- Diphenhydramine (Benadryl) 1 mg/kg IV or deep IM (Maximum dose 50 mg)
Insulin Reaction
Hypoglycemia and altered mental status due to excessive insulin
- Treat glucose < 70 mg/dl
- Dextrose 10% 0.2 gm/kg slow IV titrated to effect (max 12.5 gm) (Follow HandTevy Guide)
- If no IV/IO access Glucagon 0.5mg – 1.0 mg/kg IM/IN (Maximum dose 1mg) (Follow HandTevy Guide)
Opiates or Clonidine
- Naloxone at 0.1 mg/kg (Maximum dose 2.0 mg) via MAD, IV, IO, or IM route
Pain Management - Pediatric
Advanced Life Support
Analgesic agents may be administered if patient has severe pain and one of following:
- Isolated extremity injury
- Burn without airway, breathing, or circulatory compromise
- Typical sickle cell crisis for patient
- Animal bite or envenomation
- Agents for pain control:
- Fentanyl (Sublimaze) 1 mcg/kg (maximum 100 mcg) slow IV; repeat once after 5 minutes as needed OR 100 mcg intranasal via MAD (divide dose equally between each nare). Maximum cumulative dose is 200 mcg
- Preferentially use intranasal delivery via MAD for those where IV access may be difficult to obtain in a timely fashion
- Fentanyl (Sublimaze) 1 mcg/kg (maximum 100 mcg) slow IV; repeat once after 5 minutes as needed OR 100 mcg intranasal via MAD (divide dose equally between each nare). Maximum cumulative dose is 200 mcg
- Assess and record the patient’s pain level after medication
- Note blood pressure, mentation, and adequacy of ventilation and perfusion
- Record & monitor continuous 02 saturation and microstream capnography
Contact Medical Control for Additional Orders if Needed
Seizures – Pediatric
Basic Life Support
- Supplemental 100% oxygen if active seizures
- Blood glucose check
Advanced Life Support
- Full Pediatric ALS Assessment and Treatment
- Determine blood glucose and treat if glucose < 70 mg/dl
- Dextrose 10% 0.2 gm/kg slow IV titrated to effect (max 12.5 gm)
- If no IV available:
- Glucagon 0.5-1.0 mg/kg IM/IN (Max. 1mg)
- If hypoglycemia persists:
- Repeat blood glucose check
- Repeat Dextrose (as above) once if blood glucose < 70 mg/dl after 10 minutes
- For active seizures only, choose one of the following options:
- Do NOT delay treatment to obtain intravenous access, begin with IM dose unless IV/IO is already established
- Midazolam (Versed) 0.2 mg/kg (max 5 mg) IM or intranasal via MAD OR 0.1 mg/kg (max 2.5 mg) IV
- If seizures continue or re-occur repeat Midazolam (Versed) 0.2 mg/kg (max 5 mg) IM or intranasal via MAD OR 0.1 mg/kg (max 2.5 mg) IV; wait at least 5 minutes from initial dose
OR
- Diazepam rectal gel (Diastat®) if available: Some patients with a diagnosed seizure disorder will have their own Diazepam rectal gel (Diastat®) prescribed by their physician. When available, Diastat can be given if no IV is available. Use the patient's prescribed dose or refer to the table below. If an IV/IO is readily available, Midazolam is the preferred medication.
- Status epilepticus is defined as two or more successive seizures without a period of consciousness or recovery. This is a true emergency requiring rapid airway control, treatment, and transport.
| 2-5 years old (0.5mg/kg) | ||
| Weight | Dose | |
| (kg) | (lbs) | (mg) |
| 6-11 | 13-25 | 5 |
| 12-22 | 26-49 | 10 |
| 23-33 | 50-74 | 15 |
| 34-44 | 75-98 | 20 |
| 6-12 years old (0.3mg/kg) | ||
| Weight | Dose | |
| (kg) | (lbs) | (mg) |
| 10-18 | 22-41 | 5 |
| 19-37 | 42-82 | 10 |
| 38-55 | 83-122 | 15 |
| 56-74 | 23-164 | 20 |
Transport of Pediatric Patients
The National Highway Traffic Safety Administration (NHTSA) recommends the following for the safe transportation of children in emergency ground ambulances.
Child restraint system options for ground ambulance transport include integrated seats, conventional FMVSS 213 compliant systems for passenger vehicles, cot mounted devices, commercial pediatric immobilization devices and long board/harness immobilizer systems.
- For a child that is uninjured/not ill or a child that is ill and/or injured but does not require spinal immobilization, transport using size appropriate child restraint system that complies with FMVSS 213 secured appropriately to the stretcher or and integrated child restraint system.
- For a child whose condition requires spinal immobilization and/or lying flat, secure the patient to a size appropriate spineboard and secure the board to the stretcher head first, with three horizontal restraints across the torso (chest, waist, and knees) and a vertical restraint across each shoulder.
- For a child requiring transport as part of a multiple patient scenario (newborn with mother, multiple children, etc.) if possible transport each as a single patient according to the above protocols. For mother and newborn, transport newborn in a size appropriate FMVSS 213 compliant child restraint device in the rear-facing EMS provider seat with a forward facing belt path that prevents forward and lateral movement, leaving the stretcher for the mother.
No infant or child should be held in the parent, caregiver, or EMT’s arms or lap during transport
Contact Medical Control for Additional Orders if Needed