
COVID
Viral Alert Screening
The purpose of a Viral Alert is to provide pre-arrival Emergency Department notification in order to have a mechanism in place for hospitals to follow up with exposed crews, to inform the hospital personnel of the need to don full PPE given exposure risk, and to isolate patients into COVID specific units. A viral alert will be issued for patients who meet ANY ONE of the following criteria:
- Person has fever OR cough OR Shortness of breath OR >24 hrs of diarrhea (diarrhea has to be accompanied by other viral symptoms like body aches, fatigue, anorexia, chills)
- Person who had been tested or had been told to isolate and presumed COVID positive
- Close contact (being within approximately 6 feet) OR community contact (i.e. attended the same gathering or stayed on the same cruise ship) with a suspected/laboratory confirmed COVID-19 case
- Close contact with a person who had been told to self-isolate for possible COVID 19
- Altered mental status (unless confirmed baseline per family/caregiver)
- Cardiac Arrest
Cardiac Arrest in Suspected COVID Patients
Assume all cardiac arrest patients to be suspected COVID patients unless there was a clear inciting factor AND bystanders can answer the COVID screening for the patient (i.e. respiratory arrest from choking at a family dinner with negative screening).
Basic Life Support
· All personnel should Don full PPE (N95, eye protection, gown, double gloves) prior to physical contact with the patient
· When available, place a clear barrier over the patient (such as a rain coat) to utilize during ventilations and compressions, in order to decrease aerosolization
· Check responsiveness
· Call “Patient Contact/Working code” time to dispatch
· Utilize pit crew approach with as limited personnel as possible
· Open airway, check breathing, and feel for carotid pulse
· If a pulse is not definitely felt within 10 seconds immediately begin chest compressions while preparing to apply AED or Monitor/Defibrillator
· Assist ventilation with minimal interruptions in chest compressions
- When bagging the patient, be sure to have a very good seal in efforts to decrease exposure. This can be achieved by either utilizing the 2 hand technique or using a CPAP mask in place of the mask for the BVM
- Use a PEEP valve for the BVM when available
- Provide ventilations after 30 compressions; do not bag simultaneously with compressions. When not providing ventilations, if feasible, place a surgical mask on the patient. (No more than 3 second pauses of CPR for ventilation).
o 30:2 compression to ventilation ratio for BLS
- A LUCAS device should be used when available
· Apply AED and follow directions
· If shockable rhythm identified by AED:
o Administer shock and call “first shock” time to dispatch
o Resume CPR immediately after shock is delivered for 2 minutes
o Do not wait for pulse or rhythm check
· Re-analyze rhythm using AED and follow directions
Advanced Life Support
· Advanced airway/ventilatory management
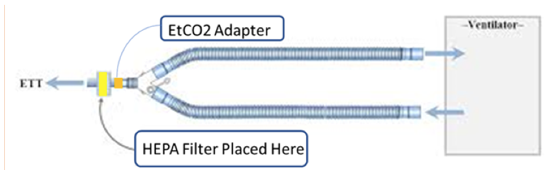
- When using a BVM, Supraglottic device, or Endotracheal tube, a viral filter must be attached PRIOR TO BAGGING. It has to be attached closest to the patient; proximal to the end tidal device.
- Utilize a Supraglottic device for airway management. It ultimately allows for less time in the airway which equates to less exposure.
SGA> INTUBATION> BVM (Most preferred to least preferred)
- Hold compressions during intubation to decrease exposure, but for no more than 10 seconds.
- If it appears the patient has a difficult airway, proceed directly to Supraglottic rather than intubation, as intubating in difficult circumstances may require more attempts= more exposure.
- Video laryngoscopy is preferred over direct laryngoscopy as it typically requires less time and allows the operator to be further away from the airway, which translates to less exposure.
o Ventilation rate with the Supraglottic or Endotracheal Tube of 8-10 per minute (avoid hyperventilation)
· If unwitnessed arrest, immediately begin CPR and continue until ready for rhythm analysis
· Follow algorithm for specific rhythm
· The Lifepack should be as far away from the patient as possible.
· Attempt peripheral IV, if unobtainable proceed to adult intraosseous access
o All medications listed for IV use can be given IO
o For medical arrests, continue high quality cardiac arrest management on scene for 20 minutes. Follow Termination of Resuscitation guidelines.
o After transfer of care or immediately following termination of resuscitation, a brief time out should be performed to identify all equipment used and secure for thorough disinfection. All crew members should carefully doff PPE at this time, under the observation of each other to identify any possible breeches.
This protocol is to be used for all viral alert patients.
Basic Life Support
- All personnel should Don full PPE (N95, eye protection, gown, double gloves) in anticipation of an aerosol generating procedure (NRB, BVM, suctioning, intubation, nebulizing treatments, CPAP) for patients with shortness of breath
- If suspicion of trauma, maintain C-spine immobilization
- If patient has access to their own inhaler, you may ask them to self- administer 4 puffs instead of providing nebulizing treatments en route.
· Minimize suction when possible
· Patients requiring supplemental O2 via nasal cannula still should wear a surgical mask
· Supplemental 100% oxygen (NRB), then NRB at 15L with the addition of a nasal cannula at 10L (when available), then BVM ventilation (with a viral filter) if persistent hypoxia or severe respiratory distress
· Monitor ETCO2 level (35-45 normal)
· Use 2 hand BVM technique to ensure adequate seal (less aerosolization). Alternatively, you can switch the BVM mask for the mask that is for CPAP use, for a tighter fit.
· Use a PEEP valve for the BVM when available
Advanced Life Support
· Reserve aerosol generating procedures for patients who have persistent hypoxia or are in severe respiratory distress
- Aerosol generating: NRB, BVM, suctioning, intubation, nebulizing treatments, CPAP
· Monitor end-tidal CO2 (capnography 35-45 normal) and ensure oxygen saturation > 94% continuously
· For hypoxia despite NRB (15L), a nasal cannula can be added (10L) to provide high flow (if available). This may be helpful in decreasing need for intubation in a hypoxic patient, if they are mentating well and are without respiratory distress.
· Invasive ventilation (Supraglottic + viral filter preferred) should be considered for the following:
o Apnea
o Decreased level of consciousness with respiratory failure (i.e. hypoxia (O2 sat <90) not improved by 100% oxygen, and/or respiratory rate < 8)
o Poor ventilatory effort (with hypoxia not improved by 100% oxygen)
o If patient is able to tolerate (no gag reflex) insertion of OPA then advanced airway should be inserted.
o When using a BVM, Supraglottic device, or Endotracheal tube, a viral filter must be attached PRIOR TO BAGGING. It has to be attached closest to the patient; proximal to the end tidal device.
o Utilize a Supraglottic device for airway management. It ultimately allows for less time in the airway which equates to less exposure.
SGA> INTUBATION> BVM (Most preferred to least preferred)
o If it appears the patient has a difficult airway, proceed directly to Supraglottic rather than intubation, as intubating in difficult circumstances may require more attempts= more exposure.
o When intubating is necessary, video laryngoscopy is preferred over direct laryngoscopy as it typically requires less time and allows the operator to be further away from the airway, which translates to less exposure.
- Attempt cricothyrotomy after all other oxygenation/ventilation methods have failed: Inability to ventilate AND inability to intubate.
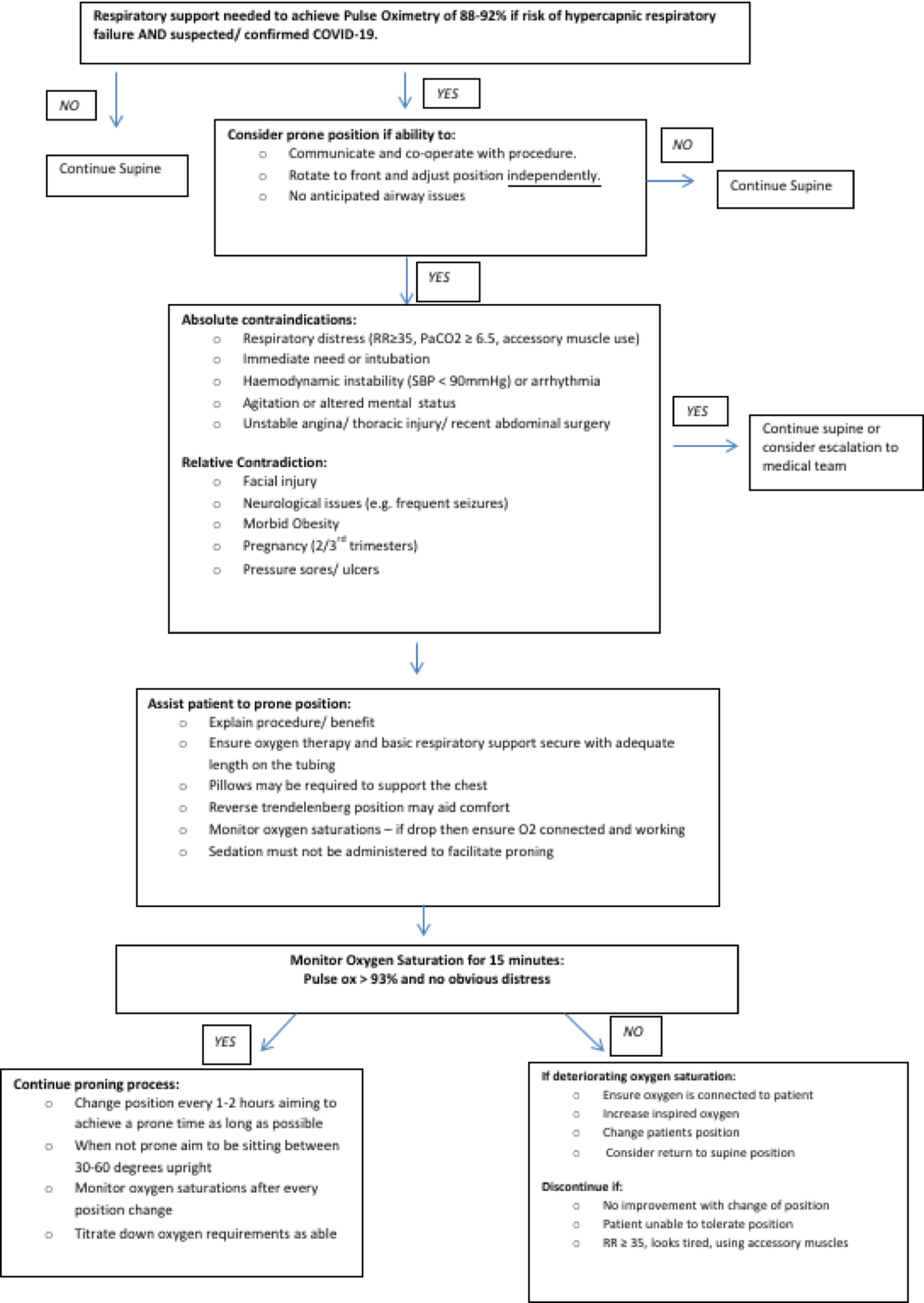
Proning
Proning improves oxygenation in patients with ARDS (acute respiratory distress syndrome) by reducing V/Q mismatch and shunting, recruiting posterior lung segments, and improving secretion clearance.
Indications (all must be present):
- Suspected or confirmed COVID-19
- Patient can participate in repositioning
- Hypoxic
Contraindications:
- Respiratory distress (RR>35, accessory muscle use)
- Altered mental status or agitation
- Hemodynamic instability (SBP<90 or arrhythmia)
- Spinal immobilization required (unstable spine or recent thoracic or abdominal surgery)
- Immediate need for intubation
Relative contraindications
- Facial injury
- Neurological issues (eg frequent seizures)
- Morbid obesity
- Pregnancy (2/3rd trimesters)
- Pressure sores/ulcers
Considerations:
- Anyone with pulse oximetry of 88-92% after application of oxygen via Non rebreather (NRB) and COVID 19 suspected
- Consider proning if patient is able to communicate and co-operate with procedure
- Is able to Rotate themselves to the front and adjust position independently
- No anticipated airway issues (including no vomiting, drooling)
Technique:
- Assist patient to prone position
- Explain procedure/benefit
- Ensure oxygen therapy and basic respiratory support secure with adequate length on the tubing
- Pillow are required to support the chest
- Reverse Trendelenburg may aid in comfort
- Monitor oxygen saturation and end tidal CO2 to ensure oxygenation and ventilation is adequate
- Sedation must not be administered

(Above picture shows proned position)

(Above picture shows lateral recumbent position)
Alternate Medical Treatment Sites for Viral Alerts
Viral Alert patients who meet the following criteria can be transported to a Free Standing Emergency Department:
- GCS 15
- Respiratory Rate <30
- Pulse Oximetry >90% on Room Air or Nasal Cannula
- No signs of shock (BP>100, ETCO2>25, HR< 130)